Prevention in dentistry does not happen solely in the operatory, it happens at home. We can remove calculus, reduce inflammation, and deliver excellent professional care, but oral health is ultimately protected in the everyday moments between visits.
A landmark study demonstrated that gingivitis can develop in as little as 2 to 3 weeks without effective plaque control, underscoring the urgency of patient participation in daily oral care.1 This reinforces a critical truth: while we as clinicians diagnose and treat disease, patients ultimately control disease prevention through their daily behaviors.
Unlike operative and restorative care, preventive care requires us to partner with patients, moving from a transactional, prescriptive model toward a patient-centered approach.
Moving beyond Tell-Show-Do for behavior change
Tell-Show-Do (TSD) has long been a familiar approach in dentistry, but its original purpose was to manage dental fear and anxiety, particularly in children, not to drive long-term behavior change. Research evaluating Tell-Show-Do confirms its effectiveness in reducing anxiety, but not in teaching self-care behaviors.2
When applied to oral hygiene instruction, starting with Tell assumes the clinician knows best and overlooks the patient’s experiences, preferences, and readiness to change. As a result, it falls short of supporting lasting adherence to preventive behaviors.
What is patient-centered care?
Patient-centered care (PCC) is defined as care that is respectful of and responsive to individual patient preferences, needs, and values, ensuring those values guide clinical decisions.3 PCC transforms oral health care into a partnership, where behavior change is co-created rather than prescribed.
Key characteristics of PCC include:3
- Respectful, trusting relationships.
- Active patient involvement.
- Non-judgmental, empathetic communication.
- Individualized care plans.
- High-quality, supportive information.
This approach is particularly important for prevention, where success depends on consistent daily behaviors at home.
Several behavioral change models have been developed to facilitate behavior change. The protocol described below represents an emerging patient-centered approach that integrates behavior change strategies into routine clinical practice.
A protocol for patient change
TePe Prevention Compass™ Protocol is a 7-step chairside approach designed to integrate behavior change into daily clinical workflow. Built on behavioral science, neuroscience, and digital support tools, it shifts care from prescriptive instruction to patient-centered collaboration. Behavior change is complex and rooted in multiple models; this protocol translates that complexity into clear, actionable steps for everyday practice.
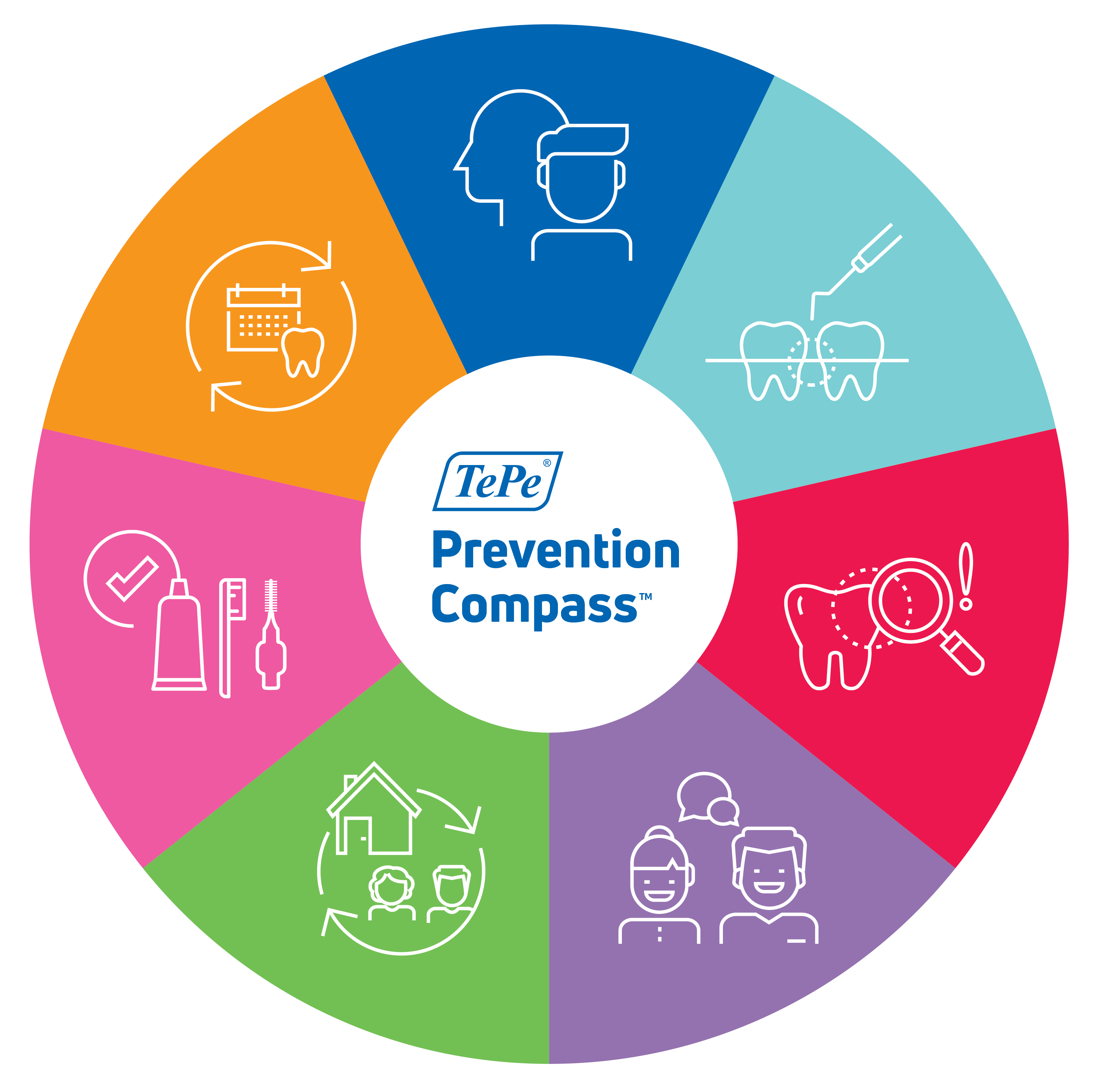
The protocol incorporates 12 behavior change models, with particular emphasis on COM-B (Capability, Opportunity, Motivation-Behavior), GPS (Goals, Planning, Self-Regulation), and motivational interviewing (MI).4-15 Other behavioral change models were used to explore a patient’s self-efficacy, perceived beliefs, control of behavior, intrinsic motivation, self-regulation, and social influences. Neuroscience explains the primary role of cues to trigger behavior, moving from a goal to true habit development.16,17 Digital tools offer a bridge between dental appointments to sustain behavior through skill building, habit formation, and increasing motivation.
The sequence includes the following steps:
- Identity – Behavior change starts first with an identity change.
- Assessment – Assess every patient using multiple modalities.
- Motivation – Make biofilm visible to highlight urgency.
- Training – Build capability by focusing on one small change.
- Environment – Consider external and social factors.
- Planning – Create a goal to initiate change that develops into lasting habits.
- Evaluation – Create a clear pathway to strengthen patient-clinician collaboration.
Here’s a closer look at each component:
I — Identity

Behavior change begins with identity. Before adopting a new habit, patients must move beyond “what to do” and instead answer: “Who do I want to be?”
Chairside Actions:
- Complete a medical and dental history.
- Explore the patient’s beliefs and attitudes toward oral health.
- Co-create a realistic “I am …” statement that reflects your patient’s identity related to their oral health.
Creating an “I am …” statement becomes a powerful psychological anchor. It directs a person’s reality, becoming their identity and behaviors follow as an extension of who they are.
Patient-Centered Prompts:
- "How does taking care of your teeth fit with the person you want to become?”
- “What kind of person do you want to be when it comes to oral health?”
Identity Examples:
- “I am a person who cares for my oral health.”
- “I am capable of keeping my gums healthy every day.”
When patients internalize this identity, behaviors like interdental cleaning become natural extensions of who they are—not forced tasks.
A — Assessment

Assessment establishes a clear understanding of your patient’s current oral health and risk factors, while building the foundation for personalized care.
Chairside Actions:
- Assess teeth, gingiva, and periodontal tissues.
- Evaluate implants and peri-implant health.
- Utilize risk assessments, digital tools, and diagnostics.
This step links clinical findings to behaviors, reinforcing that oral health outcomes are directly influenced by daily habits.
M — Motivation

Patients are more likely to change when they can see the problem. Because gingivitis and early periodontal disease can be silent, visualization is key.
Chairside Actions:
- Apply disclosing solutions to highlight plaque.
- Use intraoral photography and digital scans to show areas of concern.
- Link assessment data (i.e., bleeding, carious lesions) to areas of uncontrolled biofilm levels.
This transforms abstract risk into something tangible and emotionally meaningful, creating urgency for change.
T — Training

Training focuses on developing both knowledge and skill, ensuring patients feel confident performing the behavior at home. Rather than overwhelming patients, this step emphasizes one high-impact change.
Chairside Actions:
- Share knowledge through models, videos, demonstrations, and brochures.
- Teach home care skill and have your patient demonstrate the technique back.
- Use the teach-back technique to confirm understanding.18
- Leverage personalized technology to reinforce correct technique outside of clinic.
By focusing on one achievable change, patients gain confidence and are more likely to succeed.
E — Environment

Even motivated patients struggle if their environment creates barriers. This step addresses external and social factors that influence behavior.
Chairside Actions:
- Assess available resources, access, and time.
- Consider social influences, cultural norms, and support systems.
- Identify a cue to trigger the new behavior.
The goal is to create an environment that supports consistency.
P — Planning

Planning helps translate patient intentions into structured routines using a practical formula: Identity (“I am ...” statement) = Cue + Routine (when, where, how).
Chairside Actions:
- Focus on one small change.
- Use the formula: Identity = Cue + Routine
- Establish a cue
- Define when, where, and how the behavior will occur
- Develop a coping plan for potential barriers
Example:
- Identity: “I am someone who protects my gums.”
- Cue: After brushing at night
- Routine: Use an interdental brush in targeted areas.
This structured approach improves follow-through by reducing decision-making and reinforcing consistency.
E — Evaluation

Evaluation completes the cycle by reinforcing progress and adjusting strategies.
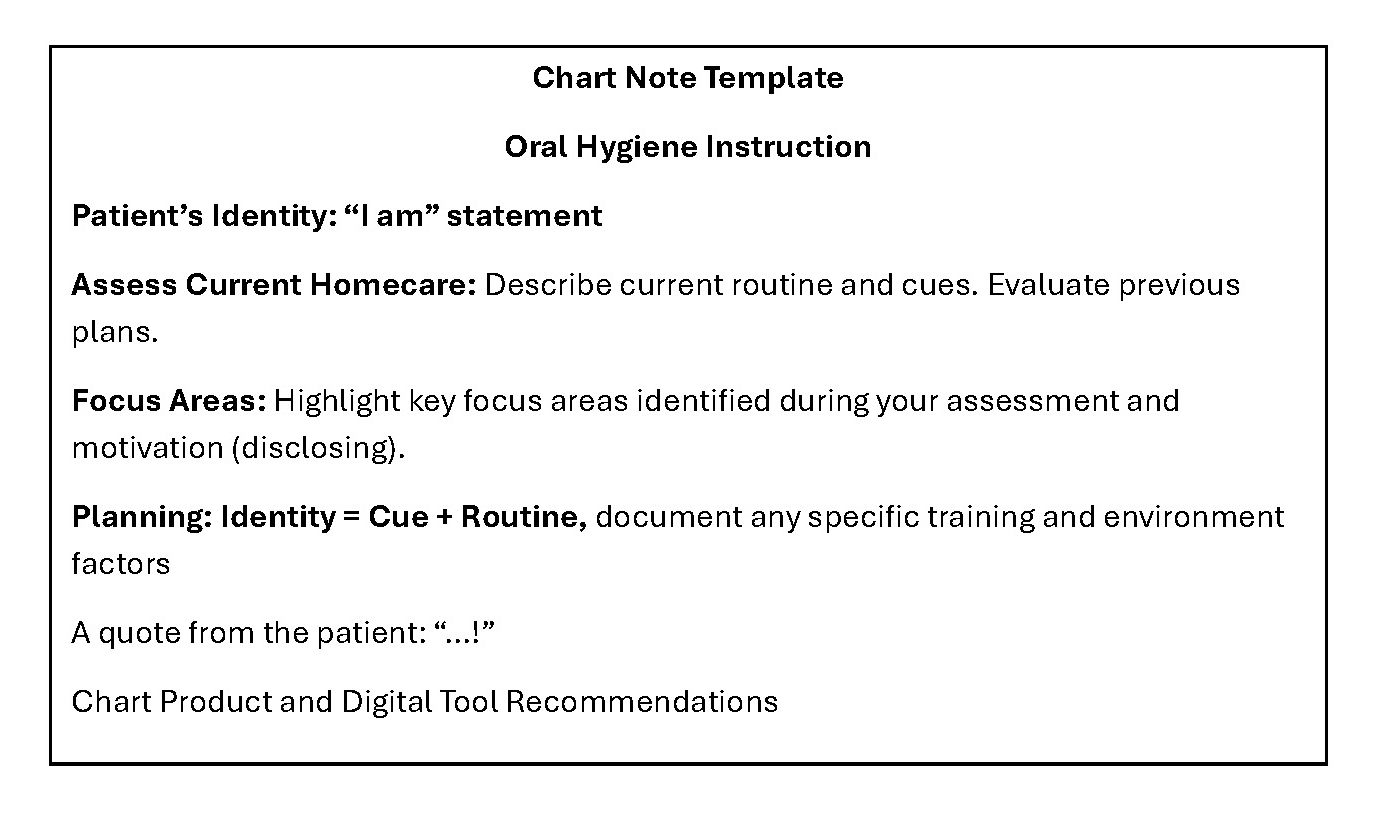
Chairside Actions:
- Review identity statements and goals.
- Monitor clinical outcomes (e.g., reduced bleeding).
- Document identity, goal (including cue), current routine, a quote from patient, and any product recommendations.
Tracking progress helps patients see improvement over time, strengthening confidence and reinforcing their identity.
Focusing on interdental cleaning
Interdental cleaning is one of the most impactful preventive behaviors because plaque accumulates most readily between teeth, where toothbrushes cannot effectively reach.
Evidence shows that adding interdental cleaning, particularly with interdental brushes, results in greater reductions in plaque and gingival inflammation compared to brushing alone.19,20 Research also demonstrates that interdental brushes often provide superior outcomes for interproximal plaque removal and periodontal health when appropriately used.21
By targeting the area where periodontal disease often begins, interdental cleaning becomes a key focus in prevention strategies.
A customized fit of an interdental brush
Effectiveness of interdental brushes depends on proper sizing. Because every interdental space is unique, a customized fit is essential.
A proper fit should include:
- Bristles uniformly contacting interproximal surfaces, reaching grooves and concavities.
- Brush circumference slightly larger than the embrasure space.
- Bristles extending under the contact point.
- Wire core not touching adjacent teeth.
- A snug feel with slight resistance, without discomfort.
To standardize sizing, manufacturers follow the ISO 16409 standard, which defines Passage Hole Diameter (PHD) as the smallest diameter through which a brush head can pass without deforming the wire core.22 While helpful, ISO sizing is only a guideline, clinical fit and patient comfort remain the priority.
The design of the brush also plays a role. The overall brush diameter is the primary determinant of cleaning effectiveness, as it dictates how well bristles adapt and reach the interproximal tooth surface. The wire diameter is equally important—it must be thin enough to pass through the space comfortably, yet stable enough to support the bristles. While bristle thickness and length influence handling and reach, research suggests they have less impact on plaque removal compared to the overall brush diameter.23-24
Individualized interdental care
Because no two interdental spaces are identical, a personalized approach is key. TePe Size Finder™ is an instrument designed to help determine the optimally sized interdental brush, making personalized oral care simple, precise, and effective.

A customized fit ensures more effective plaque removal, improved gingival health, and greater patient comfort, ultimately supporting long-term preventive success.
Conclusion
Prevention requires more than knowledge, it requires behavior change. Integrating an organized protocol can help guided behavior change fit seamlessly into a practice’s daily workflow, helping clinicians move beyond instruction to true collaboration.
By focusing on identity, building habits, and personalizing tools, like interdental brushes, we can empower our patients to take ownership of their oral health. The result is not only healthier gums but also sustainable, long-term prevention.
About the author
Heather Wong, RDH, MSDH, is Professional Relations Manager at TePe Oral Health Care. She has worked in the dental industry for more than 20 years as a clinician, educator, speaker, author, and professional relations manager. Her professional and research interests focus on oral home care and habit formation. Wong has served in leadership roles within the American Dental Hygienists’ Association at the state and local levels, including as treasurer, trustee, and delegate, and is a member of the California Dental Hygienists’ Association. She has delivered continuing education lectures for dental hygiene associations at the state, national, and international levels, as well as for organizations such as the Western Society of Periodontology, California Society of Periodontology, many study clubs, and has presented educational webinars. Heather can be reached at heather.wong@tepe.com or on Instagram @toothwisehygienist.
References
- Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36(3):177-187. doi:10.1902/jop.1965.36.3.177
- Elicherla NR, Saikiran KV, Anchala K, Elicherla SR, Nuvvula S. Evaluation of the effectiveness of tell-show-do and ask-tell-ask in the management of dental fear and anxiety: a double-blinded randomized controlled trial. J Dent Anesth Pain Med. 2024;24(1):57-65. doi:10.17245/jdapm.2024.24.1.57
- Mills I, Frost J, Cooper C, Moles DR, Kay E. Patient-centred care in general dental practice: a systematic review of the literature. BMC Oral Health. 2014;14:64. doi:10.1186/1472-6837-14-64
- Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
- Newton JT, Asimakopoulou K. Managing oral hygiene as a risk factor for periodontal disease: a systematic review of psychological approaches to behaviour change for improved plaque control in periodontal management. J Clin Periodontol. 2015;42(Suppl 16):S36-S46. doi:10.1111/jcpe.12356
- Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY: Guilford Press; 1991
- Rosenstock IM. Historical origins of the Health Belief Model. Health Educ Monogr. 1974;2(4):328-335
- Rotter JB. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr. 1966;80(1):1-28
- Leventhal H. Findings and theory in the study of fear communications. In: Advances in Experimental Social Psychology. Vol 5. Academic Press; 1970:119-186
- Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975
- Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179-211
- Bandura A. Social Learning Theory. Englewood Cliffs, NJ: Prentice-Hall; 1977
- Bandura A. Self-Efficacy: The Exercise of Control. New York, NY: W.H. Freeman; 1997
- Deci EL, Ryan RM. Intrinsic Motivation and Self-Determination in Human Behavior. New York, NY: Springer; 1985
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390-395. doi:10.1037/0022-006X.51.3.390
- Graybiel AM. Habits, rituals, and the evaluative brain. Annu Rev Neurosci. 2008;31:359-387. doi:10.1146/annurev.neuro.29.051605.112851
- Duhigg C. The Power of Habit: Why We Do What We Do in Life and Business. New York, NY: Random House; 2012
- Talevski J, Wong Shee A, Rasmussen B, Kemp G, Beauchamp A. Teach-back: a systematic review of implementation and impacts. PLoS One. 2020;15(4):e0231350. doi:10.1371/journal.pone.0231350
- Sälzer S, Slot DE, van der Weijden FA, Dörfer CE. Efficacy of inter-dental mechanical plaque control in managing gingivitis: a meta-review. J Clin Periodontol. 2015;42(Suppl 16):S92-S105. doi:10.1111/jcpe.12363
- Worthington HV, MacDonald L, Poklepovic Pericic T, et al. Home use of interdental cleaning devices, in addition to toothbrushing, for preventing and controlling periodontal diseases and dental caries. Cochrane Database Syst Rev. 2019;4(4):CD012018. doi:10.1002/14651858.CD012018.pub2
- Kotsakis GA, Lian Q, Ioannou AL, Michalowicz BS, John MT, Chu H. A network meta-analysis of interproximal oral hygiene methods in the reduction of clinical indices of inflammation. J Periodontol. 2018;89(5):558-570. doi:10.1002/JPER.17-0368
- International Organization for Standardization. ISO 15409:2016 Dentistry—oral hygiene products—manual interdental brushes. Geneva, Switzerland: ISO; 2016. Accessed May 26, 2026. https://www.iso.org/standard/65258.html
- Wolffe GN. An evaluation of proximal surface cleansing agents. J Clin Periodontol. 1976;3(3):148-156. doi:10.1111/j.1600-051x.1976.tb01862.x
- Staehle HJ, Sekundo C. History of interdental brushes: origins, developments, perspectives. Oral Health Prev Dent. 2025;23:1-20. doi:10.3290/j.ohpd.c_1800
